
With small clusters of COVID-19 popping up at schools and perhaps elsewhere, including the Portsmouth Naval Shipyard, New Hampshire’s pandemic situation remains, shall we say, unsettled.
But nothing worse than that – at least, not so far.
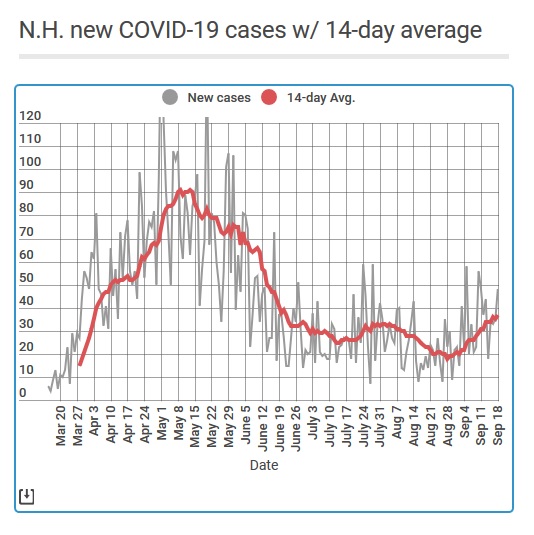
The average number of new cases in the state continues to rise slowly, but Dr. Benjamin Chan, state epidemiologist, argued Thursday that this was a reflection of much increased testing at schools and colleges.
“We are not, however, seeing a new surge in New Hampshire,” he said during a press briefing, pointing to the continued very low number of new hospitalizations in the state.
If these outbreaks remain small and stay contained in each location, then even a continued rise in total cases wouldn’t be too alarming, because it wouldn’t say that the disease is spreading through the general population.
How can we know if a rise is cases isn’t spreading? With Chan’s comment in mind, I’m going to add a fifth metric to the Monitor’s weekly measure of the pandemic’s status in New Hampshire: The number of new hospitalizations related to COVID-19 each day.
I have been tracking this number all along and now seems a good time to include it as an indication of whether we are transitioning back to a more serious phase of the pandemic.
So here is this week’s tally:
Goal 1: No sustained increase in number of new hospitalizations related to COVID-19. Have we met this goal? Yes.
In late May, almost eight people a day on average were being hospitalized because of COVID-19. The actual figure was even higher because the state adjusted figures in mid-July, adding 74 hospitalizations that had been incorrectly labeled in the database.
By the start of August that two-week average was below two new hospitalizations a day, and this month it has consistently been below a single person sent to the hospital in New Hampshire because of the SARS CoV-2 virus. As of Saturday, only eight people total were in the hospital due to COVID-19 in the state.
On a similar note, COVID-related deaths have gone way down. The current average is less than one a day, a sign of how outbreaks in long-term care facilities have been brought under control.
Goal 2: A two-week drop in new cases. Have we met this goal? No.
I average the daily new-case numbers over two weeks, to smooth out the effect of reporting delays. (Many other places average them over a single week, which explains occasional discrepancies between their conclusions and mine.)
The two-week average was 18 on Aug. 28 but has consistently edged up since then. By Friday, Sept. 18, it had doubled to 37 new cases a day, fueled by those outbreaks mentioned above.
Goal 3: Fewer than four new cases per 100,000 people each day, or 54 new cases a day. Have we met this goal? Yes.
Even with the increase we’ve been seeing, our number of new cases has for months stayed below this level, which is commonly used as a sign of widespread infection.
Goal 4: Conducting at least 150 PCR tests per 100,000 people each day, or 2,000 tests per day. Have we met this goal? Yes.
The average number of test results reported each day was about 3,500 last week, thanks to increased testing at schools and colleges.
However, we need to keep testing all over the state for anybody who asks for it. That’s the only way we’ll know what’s actually going on.
Goal 5: A positive rate of PCR tests below 5%, indicating that the virus is not spreading rapidly in the general population. Have we met this goal? Yes.
As measured by the Department of Health and Human Services, the positive rate has been below 3% for most of the summer.
I update three charts about the virus in New Hampshire each weekday: New cases, new hospitalizations, and total deaths.
 Return to the Concord Monitor
Return to the Concord Monitor
I question #5:
It’s important to note that this “Positivity” rating is not necessarily a great, leading metric/ indication of if the virus is spreading or not. (And it’s often misattributed to this). What is *IS* useful for, is gauging weather we believe there are enough tests being done. i.e. If you have an exceedingly high positivity rate – (let’s say 100% just as an example) – this means that your testing isn’t giving you conclusive information, because you could have 2x or 1000x as many actual positive people – there is no way to know.
So the real importance of this metric is actually if you have a test rate below 5%, it’s commonly (arguably) believed that you’re doing enough testing to accurately sample enough people, both positive AND negative – to get a decent read on actual positive cases. And considering about the ones you’ve missed – you numbers are probably good about +/- 5%.
Good point. I’m tweaking the word in the upcoming tracker.
Thank you for adding hospitalizations. I recall the Governor saying early on that hospitalizations were his most reliable measure of how we are doing. I think he is correct. However, people do get very sick and may suffer long-term damage without needIng hospitalization. If the virus is concentrated in nursing homes again, sick people there may die at their care facility rather than in a hospital. So hospitalizations don’t accurately measure the extent of harm, but they are a good indications of trends.
The state graph of new cases is somewhat confusing in that it adds “note:not all confirmed cases are included in this figure due to the person having an unclear onset date or no onset date because they did not experience any symptoms.”
Does this mean that they are NOT including asymptomatic cases from the date they are diagnosed via testing in this chart? A range of date of onset can be extrapolated by known data (median time to onset after exposure is 4-5 days.) Since 40% of “cases” may be asymptomatic, and since asymptomatic cases are known to transmit virus, why are asymptomatic cases not being included, and how many such cases exist relative to overall reported cases? Is this the standard for reporting sars-2-cov cases?
I suspect that means people who tested positive on the antibody test in a way that confirmed they had COVID, but it’s not clean when – or where.